Author: Daniel M. Jarvis
Affiliation: Tactical Resiliency USA / Healing the Hero USA
Abstract
This de-identified case study examines rapid psychological, cognitive, and neurophysiological changes in a 47-year-old Caucasian male Army Combat Veteran (ACV) following three sessions of Trauma Resiliency Protocol–Peer Rescue (TRP-PR), a non-prolonged trauma processing intervention designed to reduce the emotional burden of unresolved traumatic experiences without requiring extensive verbal exposure. The participant presented with severe posttraumatic stress symptoms, severe depression, severe anxiety, daily suicidal ideation, and measurable cognitive inefficiencies prior to treatment. Baseline psychometric scores were elevated across all clinical domains (Posttraumatic Stress Disorder Checklist for DSM-5 [PCL-5] = 74; Patient Health Questionnaire-9 [PHQ-9] = 23; Generalized Anxiety Disorder-7 [GAD-7] = 21). Baseline neurocognitive screening using the Evoke Neuroscience electroencephalography (EEG) platform demonstrated a global score of 33%, slowed reaction time, elevated omission errors, delayed event-related potential (ERP) latencies, and reduced heart rate variability (HRV). Following three TRP-PR sessions, self-reported symptom scores decreased to zero across all measures, suicidal ideation resolved, and global neurocognitive performance improved to 91%. EEG and ERP findings suggested partial normalization of cortical organization and improved information-processing efficiency. HRV findings remained mixed, highlighting the complexity of recovery across systems. This case supports further structured investigation into TRP-PR as a rapid-response intervention for severe combat trauma and moral injury.
Keywords: combat trauma, moral injury, TRP-PR, trauma recovery, veteran mental health, EEG, Evoke Neuroscience, HRV
Introduction
Combat trauma and moral injury remain significant contributors to psychological distress, suicidal ideation, and functional impairment among military veterans (Litz et al., 2009; Maguen & Litz, 2012). While evidence-based treatments such as prolonged exposure and cognitive processing therapy have demonstrated benefit for many individuals, barriers to treatment remain substantial, particularly among veterans who avoid care due to stigma, fear of re-exposure, or concern about professional consequences (Steenkamp et al., 2015).
Moral injury, in particular, may involve profound guilt, grief, shame, or existential conflict following exposure to events that violate deeply held values or identity structures (Litz et al., 2009). Such injuries may persist even when an individual’s actions were tactically necessary, lawful, or consistent with duty requirements.
Rapid, non-prolonged interventions that target emotional intensity, maladaptive sensory-emotional linkage, and unresolved trauma-related physiological activation may offer a useful adjunct or alternative for select high-risk populations.
Trauma Resiliency Protocol–Peer Rescue (TRP-PR) is a structured, non-clinical trauma processing intervention designed to reduce the emotional intensity associated with unresolved traumatic experiences while minimizing prolonged narrative exposure. The protocol emphasizes dissociation from distressing sensory imagery, emotional reconsolidation, reframing, and restoration of adaptive cognitive-emotional organization.
The present case study examines psychometric, neurocognitive, ERP, HRV, and quantitative electroencephalography (qEEG) changes in a combat veteran following three TRP-PR sessions. Neurophysiological assessment was conducted using the Evoke Neuroscience system, which integrates EEG, ERP, ECG, and neurocognitive screener measures to evaluate cortical timing, attentional processing, autonomic regulation, and functional performance.
Method
Participant
The participant was a de-identified 47-year-old Caucasian male combat veteran (ACV) with prior U.S. Navy service and subsequent U.S. Army service. He deployed to Iraq in 2005 and experienced a severe combat-related morally injurious event while serving in a guard tower. During the incident, he engaged a child who breached the base perimeter and posed an immediate threat under Rules of Engagement (ROE). Although the action was consistent with force protection requirements, the event resulted in enduring guilt, intrusive memories, emotional dysregulation, chronic suicidal ideation, and severe functional distress.
Measures
Psychometric Measures
- Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5)
- Patient Health Questionnaire-9 (PHQ-9)
- Generalized Anxiety Disorder-7 (GAD-7)
Neurophysiological Assessment
Neurophysiological and cognitive data were collected using the Evoke Neuroscience system (Evoke Neuroscience, Inc.), which includes:
- quantitative electroencephalography (qEEG)
- event-related potentials (ERPs)
- ECG-based heart rate variability (HRV)
- computerized neurocognitive screener
The Evoke platform was selected because it allows for simultaneous assessment of:
- cognitive processing speed
- attentional efficiency
- omission / commission errors
- cortical electrical organization
- autonomic nervous system flexibility
Procedure
The participant completed baseline psychometric and Evoke Neuroscience assessments prior to intervention. He then completed three sessions of TRP-PR focused on traumatic memory desensitization, emotional reconsolidation, and autonomic down-regulation. Follow-up psychometric and Evoke assessments were conducted after treatment.
Results
Case Study: Army Combat Veteran (ACV)
Executive Summary
This white paper presents a de-identified case study of a 47-year-old Caucasian male Army Combat Veteran (ACV) with severe combat-related traumatic stress, chronic suicidal ideation, severe depression, and debilitating anxiety. Prior to intervention, the ACV reported daily suicidal thoughts, intrusive traumatic memories, emotional dysregulation, and substantial functional impairment.
Following just three sessions of the Trauma Resiliency Protocol–Peer Rescue (TRP-PR), the ACV demonstrated complete resolution of self-reported trauma symptoms on validated psychometric measures, with substantial improvement in neurocognitive performance and measurable changes in electrophysiological markers. This case highlights the potential for rapid, non-content-intensive trauma resolution in high-risk populations.
1. Background and Subject Profile
Demographics
- Participant ID: ACV (De-identified)
- Age: 47 years old at baseline
- Sex: Male
- Race/Ethnicity: Caucasian
- Military Background: Prior U.S. Navy service; later served in the U.S. Army
- Combat Deployment: Iraq, 2005 with the Army
- Trauma Exposure: Combat-related moral injury and life-threatening operational stress
Index Trauma
During deployment in Iraq in 2005, while serving in a guard tower under established Rules of Engagement (ROE), the ACV was forced to engage and fatally shoot a five-year-old child who breached the security perimeter and posed a threat to base safety. Although the action was consistent with military ROE and force protection requirements, the event resulted in profound moral injury, intrusive recall, emotional distress, guilt, hypervigilance, and long-term psychological suffering.
Presenting Symptoms (Pre-Intervention)
Before treatment, the ACV reported:
- Daily suicidal ideation
- Severe combat-related intrusive memories
- Hyperarousal and chronic anxiety
- Severe depressive symptoms
- Anger dysregulation
- Sleep disruption
- Emotional numbness and avoidance
- Cognitive slowing and impaired concentration
2. Pre-Intervention Clinical and Neurophysiological Assessment
Psychometric Baseline Scores
| Measure | Pre-Treatment Score | Clinical Interpretation |
| PCL-5 | 74 | Extremely elevated trauma burden |
| PHQ-9 | 23 | Severe depressive symptom load |
| GAD-7 | 21 | Severe anxiety symptom load |
Suicide Risk and Functional Burden
Before treatment, the ACV reported thinking about suicide every day. In operational terms, this represents a high-risk pre-intervention presentation, especially when combined with severe trauma symptoms, severe depression, severe anxiety, impaired affect regulation, slowed reaction time, and cognitive inconsistency. The case is notable not simply because symptoms were present, but because the overall pattern suggested a system under sustained threat load—psychologically, cognitively, and physiologically.
Baseline Neurocognitive Performance
Global Neurocognitive Score: 33%
This baseline score reflected broad impairment across multiple domains rather than a narrow deficit profile. The most impaired areas were those most relevant to post-traumatic suffering: affect regulation, memory performance, sensory integration, motor output, and language fluency.
Domain Breakdown at Baseline
| Domain | Pre Score |
| Memory | 38% |
| Executive & Attention | 67% |
| Word Fluency | 25% |
| Affect | 13% |
| Sensory | 17% |
| Motor | 21% |
Baseline Memory Subtypes
| Memory Subtype | Pre Score |
| Spatial Navigation | 67% |
| Temporal Orientation | 50% |
| Procedural Actions | 50% |
| Episodic Memory for Places | 25% |
| Face Recognition | 0% |
| Semantic Word Knowledge | 25% |
This pattern is consistent with trauma burden disrupting both efficient recall and emotionally neutral cognitive processing. Particularly notable are the low scores in episodic memory for places, semantic word knowledge, and face recognition, suggesting possible interference between emotional load and routine cognitive throughput.
Baseline Response Metrics
| Metric | Pre Result | Interpretation |
| Response Speed | 781 ms | Markedly slowed processing speed |
| Response Consistency (variance) | 93 ms | Poor sustained attentional stability |
| Missed Response (omission) | 28.57% | High inattention / missed targets |
| Wrong Response (commission) | 1.63% | Relatively preserved inhibitory control |
Taken together, these metrics suggest that the ACV was not merely distressed, but functionally burdened in ways that could affect daily decision-making, reaction efficiency, attention, and performance reliability.
Baseline ERP Findings
Event-Related Potentials (ERPs) provide a time-sensitive look at how the brain is processing incoming information.
P300a (Attention / Orienting to Salient Stimuli)
- Latency: 484 ms
- Power: 14.0 µV
The delayed latency suggests slowed attentional orienting to relevant stimuli, even though amplitude remained preserved.
P300b (Information Processing / Working Memory Updating)
- Latency: 588 ms
- Power: 22.6 µV
This markedly slowed latency is consistent with delayed cognitive updating and burdened information processing.
N100 (Early Visual-Sensory Processing)
- Latency: 288 ms
- Power: -12.2 µV
This slower-than-reference early sensory response suggests delayed initial visual processing.
Baseline HRV / Autonomic Findings
| Metric | Pre Result | Reference Meaning |
| Heart Rate | 80 bpm | Upper end of stated reference range |
| SDNN | 42 ms | Reduced autonomic flexibility |
| Total Power | 649 ms² | Below optimal autonomic reserve |
At baseline, autonomic regulation appeared constrained, consistent with chronic stress load and reduced recovery capacity.
Baseline qEEG / Eyes Closed Brain Mapping
Figure 1. Pre-Treatment Eyes Closed qEEG Brain Map (Posterior / Posterior Temporal View)
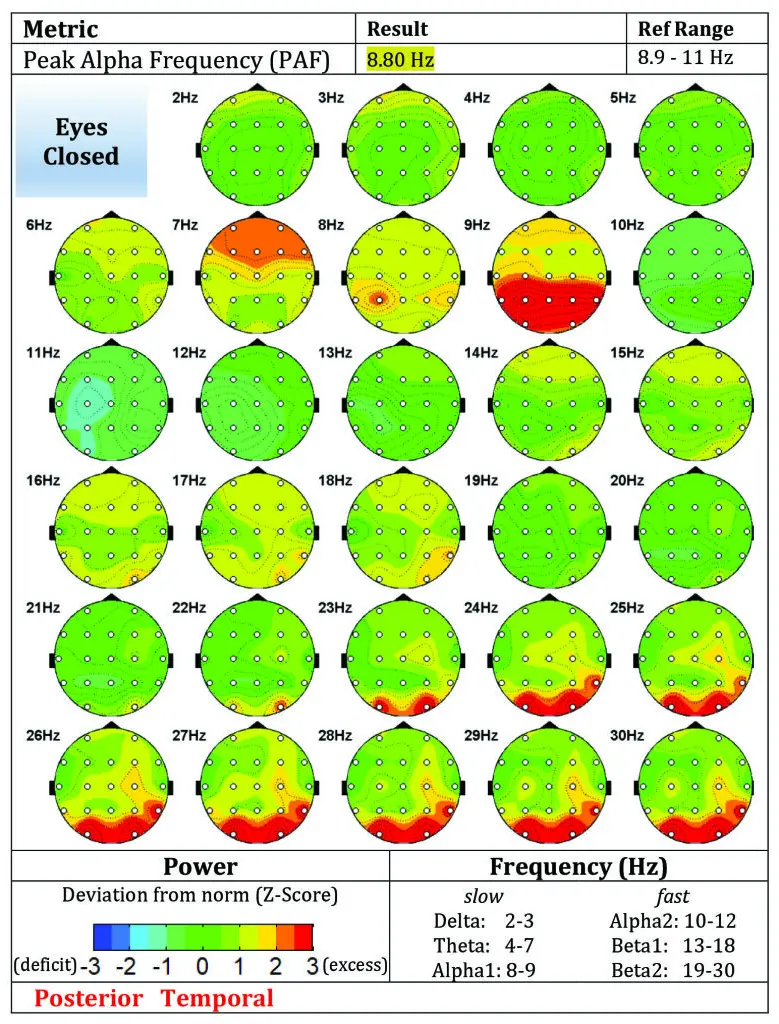
Figure Caption: Baseline eyes-closed qEEG map demonstrating elevated posterior and posterior-temporal dysregulation, with excess activity patterns involving regions associated with salience monitoring, emotional memory processing, and threat-related internal scanning.
At baseline, the eyes-closed maps showed elevated posterior and posterior-temporal abnormalities, including deviations involving the posterior cingulate, cuneus, and superior temporal regions. In plain language, these are areas often associated with internal monitoring, evaluative processing, visual-emotional integration, salience detection, and memory-linked processing. The overall pattern is consistent with a brain that may be spending too much energy scanning, evaluating, and reprocessing emotionally loaded material.
Baseline Clinical Interpretation
The pre-treatment profile showed convergence across four levels:
- Subjective distress: severe PTSD, depression, anxiety, and daily suicidal ideation.
- Functional cognition: low global cognitive score with slowed reaction time and high omission errors.
- Neuroelectric timing: delayed ERP responses indicating slowed attentional and information-processing speed.
- Autonomic strain: low HRV markers suggesting reduced physiological flexibility.
In combination, these findings describe a combat veteran under heavy and persistent allostatic load.
3. TRP-PR Intervention Protocol
Treatment Overview
The ACV completed three sessions of Trauma Resiliency Protocol–Peer Rescue (TRP-PR).
Core Treatment Objectives
The intervention was aimed at reducing the emotional charge tied to the traumatic memory, interrupting maladaptive sensory-emotional linkage, and restoring more adaptive cognitive and physiological organization without requiring prolonged trauma narration.
Protocol Features Used in This Case
- Guided dissociation from traumatic imagery
- Reduction of sensory-emotional intensity
- Memory reconsolidation strategies
- Reframing of emotional meaning
- Future pacing and state stabilization
- Non-prolonged, non-exposure-based processing
Why This Matters
This case is clinically significant because the presenting trauma involved both combat exposure and moral injury. The latter often persists even when a service member understands that their action was lawful, tactically necessary, and compliant with ROE. TRP-PR in this context was not simply targeting fear-based recall; it was targeting the enduring emotional injury linked to guilt, grief, and identity-level distress.
4. Post-Intervention Outcomes
Psychometric Outcomes
| Measure | Pre | Post | Absolute Change | Relative Change |
| PCL-5 | 74 | 0 | -74 | 100% reduction |
| PHQ-9 | 23 | 0 | -23 | 100% reduction |
| GAD-7 | 21 | 0 | -21 | 100% reduction |
Suicide Risk Outcome
The ACV reported daily suicidal thinking before treatment and no longer reported suicidal thinking after treatment. From a clinical-risk standpoint, that is one of the most meaningful changes in the case.
Post-Treatment Neurocognitive Performance
Global Neurocognitive Score: 91%
Post-Treatment Domain Breakdown
| Domain | Pre | Post | Change |
| Memory | 38% | 93% | +55 |
| Executive & Attention | 67% | 100% | +33 |
| Word Fluency | 25% | 88% | +63 |
| Affect | 13% | 96% | +83 |
| Sensory | 17% | 88% | +71 |
| Motor | 21% | 79% | +58 |
| Global Score | 33% | 91% | +58 |
Post-Treatment Memory Subtypes
| Memory Subtype | Pre | Post | Change |
| Spatial Navigation | 67% | 100% | +33 |
| Temporal Orientation | 50% | 75% | +25 |
| Procedural Actions | 50% | 100% | +50 |
| Episodic Memory for Places | 25% | 100% | +75 |
| Face Recognition | 0% | 83% | +83 |
| Semantic Word Knowledge | 25% | 100% | +75 |
This is not a subtle shift. It reflects a broad restoration of cognitive performance across memory organization, language-related throughput, emotional regulation, and sensory-motor efficiency.
Post-Treatment Response Metrics
| Metric | Pre | Post | Change |
| Response Speed | 781ms | 499ms | 282ms faster |
| Response Consistency | 93ms | 22ms | 71ms improvement |
| Missed Response | 28.57% | 0.00% | Eliminated |
| Wrong Response | 1.63% | 2.04% | Small increase, still within range |
These shifts suggest markedly improved attention, engagement, and processing efficiency after treatment.
Post-Treatment ERP Findings
| ERP Metric | Pre | Post | Direction |
| P300a Speed | 484 ms | 560 ms | Slower |
| P300a Power | 14.0 µV | 15.9 µV | Higher |
| P300b Speed | 588 ms | 552 ms | Faster |
| P300b Power | 22.6 µV | 27.2 µV | Higher |
| N100 Speed | 288 ms | 280 ms | Faster |
| N100 Power | -12.2 µV | -12.6 µV | Slightly stronger |
ERP Interpretation
The ERP picture is mixed but still informative. P300b and N100 moved in a favorable direction, suggesting improved downstream information processing and slightly improved early sensory timing. P300a latency, however, became slower despite increased amplitude. This may indicate that not every electrophysiological marker normalized at the same pace as symptom relief and cognitive performance. In other words, the veteran’s subjective and functional recovery appears to have outpaced complete normalization of all ERP timing markers.
That is not uncommon in recovery work. Different systems often recover on different timelines.
Post-Treatment HRV / Autonomic Findings
| Metric | Pre | Post | Direction |
| Heart Rate | 80 bpm | 98 bpm | Higher |
| SDNN | 42ms | 28ms | Lower |
| Total Power | 649ms² | 191ms² | Lower |
Autonomic Interpretation
The HRV findings are important because they add nuance. Unlike the symptom scales and neurocognitive screener, HRV did not improve in this post-treatment scan and instead moved in a less favorable direction.
Possible explanations include:
- scan-day stress or arousal
- sleep disruption prior to testing
- stimulant use, nicotine, caffeine, illness, or dehydration
- residual sympathetic activation unrelated to the trauma target itself
- physical conditioning factors
- temporal spacing of the follow-up scan relative to recent life stressors
This matters because it prevents overclaiming. The case strongly supports major subjective and cognitive recovery, but it does not support the conclusion that every physiological recovery marker normalized in parallel.
Post-Treatment qEEG / Eyes Closed Brain Mapping
Figure 2. Post-Treatment Eyes Closed qEEG Brain Map (Posterior View)
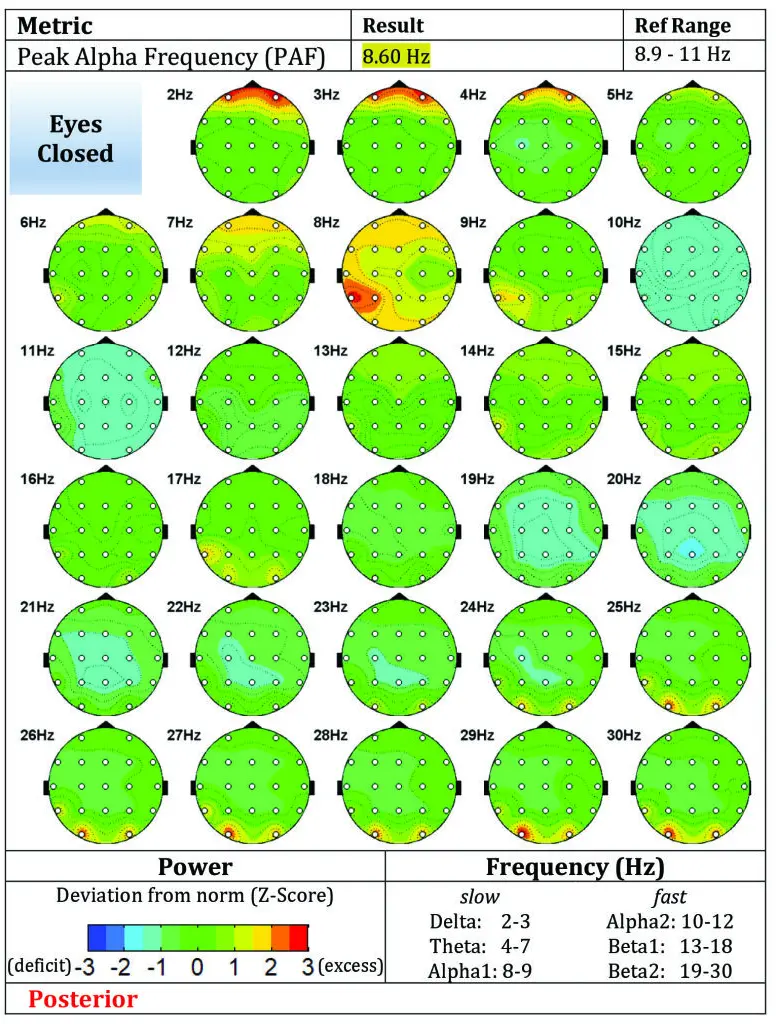
Figure Caption: Post-treatment eyes-closed qEEG map demonstrating improved cortical organization, reduced posterior excess activity, and a more stable electrophysiological profile following three sessions of TRP-PR.
The post-treatment eyes-closed maps appear more organized overall, with less dramatic posterior excess across multiple frequencies and a more stable-looking distribution than the baseline record. Some deviations remain, but the overall electrophysiological picture appears less burdened by the same degree of widespread posterior/posterior-temporal excess seen in the baseline scan.
Baseline Callout:
- Severe symptom burden
- Daily suicidal ideation
- Global score: 33%
- Delayed processing and high omission errors
Post-Treatment Callout:
- No reported suicidal ideation
- PCL-5: 0
- PHQ-9: 0
- GAD-7: 0
- Global score: 91%
5. Comparative Analysis
Symptom Burden
The most striking result in this case is total reported elimination of trauma, depression, and anxiety symptoms on the three screening instruments used. Going from PCL-5 74 to 0, PHQ-9 23 to 0, and GAD-7 21 to 0 after three sessions is an unusually large change and represents a full subjective remission signal within the confines of this case study.
Cognitive Performance
The cognitive screener shows that the veteran did not merely feel better; he also performed better. Memory, affect, language fluency, and sensory-motor domains all rose dramatically, while omission errors dropped to zero and reaction time normalized into the stated reference band.
Moral Injury Considerations
This case may be especially relevant to moral injury populations. The traumatic event was not framed as personal failure in the tactical sense; the ACV acted under ROE to protect the base. Yet the emotional injury persisted. This distinction is important. Many veterans do not suffer solely because of fear-based trauma. They suffer because the event violated deeply held beliefs about innocence, duty, identity, or what it means to live with one’s own actions after war.
TRP-PR may have particular relevance where the wound is not only fear, but meaning.
What Improved Fast vs. What Lagged
Improved rapidly:
- self-reported trauma burden
- depression burden
- anxiety burden
- suicidal ideation
- cognitive score
- omission errors
- reaction time
- several ERP measures
Lagged or remained mixed:
- P300a latency
- HRV measures
- peak alpha frequency remained slightly below reference on both scans
This pattern suggests that symptom relief and functional recovery may emerge before full autonomic or electrophysiological normalization.
6. Operational and Clinical Significance
For veteran-serving organizations, this case has several implications.
- Speed Matters
When an individual presents with severe symptoms and daily suicidal thinking, interventions that can produce meaningful change quickly have obvious value. - Non-Prolonged Trauma Processing May Reduce Barriers
Veterans often avoid care that requires prolonged retelling of traumatic events. A method that reduces emotional intensity without forcing extensive disclosure may improve uptake. - Objective Measurement Strengthens Credibility
Using pre/post psychometrics together with qEEG, ERP, and HRV data offers a stronger evidence narrative than symptom reporting alone. - Recovery Is Multidimensional
This case shows why it is useful to measure more than one system. The psychometrics and neurocognitive domains improved dramatically, while HRV remained impaired. That does not invalidate the gains; it clarifies where continued optimization may still be needed.
7. Limitations
This is a single de-identified case study and should not be generalized beyond its scope.
Key limitations include:
- single-subject design
- no control condition
- no randomization
- no blinded assessment
- limited longitudinal follow-up in this report
- possible confounders affecting HRV and scan-day physiology
- psychometric scores were reported as outcome data but broader functional measures were not included here
The magnitude of change is compelling, but future structured research should examine durability, replication, subgroup effects, and comparative performance against other approaches.
Discussion
This case demonstrates clinically meaningful change across multiple domains following a brief three-session TRP-PR intervention. Most notable was the complete reduction in self-reported PTSD, depression, and anxiety symptoms, along with resolution of daily suicidal ideation. Given the participant’s severe pre-treatment symptom burden and moral injury-related trauma, the magnitude of change warrants attention.
From a neurocognitive standpoint, the increase in global performance from 33% to 91% suggests broad functional restoration. Improvements in memory, word fluency, affective regulation, and sensory-motor processing support the possibility that reducing unresolved trauma burden may improve cognitive efficiency.
ERP findings provided partial support for improved cortical timing and information processing, particularly in P300b and N100 measures. The qEEG findings also suggested a more organized post-treatment cortical profile, especially in posterior regions implicated in salience monitoring and memory-linked processing.
However, HRV findings remained mixed and, in some respects, less favorable at follow-up. This discrepancy is important. Trauma recovery is not always linear across all biological systems, and improvements in emotional burden may precede full autonomic normalization. Factors such as sleep, scan-day arousal, recent life stressors, and physical conditioning may have influenced HRV outcomes.
This case also has relevance for moral injury. The participant’s trauma involved an event that was operationally justified but emotionally devastating. The persistence of suffering despite tactical necessity aligns with prior literature showing that moral injury is often rooted in unresolved meaning, grief, and self-perception rather than fear alone (Litz et al., 2009).
Limitations
This report is limited by its single-case design, lack of control condition, and absence of long-term follow-up in the current manuscript. Findings should be interpreted as preliminary and hypothesis-generating rather than definitive evidence of efficacy.
Future Directions
Future research should examine:
- replication in larger veteran samples
- durability of symptom reduction over time
- comparison with standard trauma interventions
- subgroup analyses for moral injury presentations
- multimodal biomarker tracking
Conclusion
This de-identified Army Combat Veteran case presents a striking example of rapid change following three sessions of TRP-PR. Before treatment, the ACV exhibited severe trauma burden, severe depression, severe anxiety, daily suicidal ideation, marked neurocognitive inefficiency, delayed ERP timing, and reduced autonomic flexibility. After treatment, symptom scores fell to zero, suicidal ideation resolved, cognitive performance increased dramatically, omission errors were eliminated, and multiple electrophysiological indicators improved.
At the same time, the HRV profile reminds us that human recovery is not always linear or uniform across all systems. That nuance strengthens, rather than weakens, the value of this case. The findings suggest that TRP-PR may be capable of producing rapid relief in severe combat- and moral-injury presentations, while also highlighting the importance of continued follow-up and multi-domain measurement.
For organizations serving veterans, first responders, and other high-risk populations, this case supports deeper formal investigation into TRP-PR as a rapid-response intervention for unresolved trauma and suicidal suffering.
References
Evoke Neuroscience. (n.d.). Evoke EEG system user manual.
Litz, B. T., Stein, N., Delaney, E., Lebowitz, L., Nash, W. P., Silva, C., & Maguen, S. (2009). Moral injury and moral repair in war veterans: A preliminary model and intervention strategy. Clinical Psychology Review, 29(8), 695–706.
Maguen, S., & Litz, B. T. (2012). Moral injury in veterans of war. PTSD Research Quarterly, 23(1), 1–6.
Steenkamp, M. M., Litz, B. T., Hoge, C. W., & Marmar, C. R. (2015). Psychotherapy for military-related PTSD: A review of randomized clinical trials. JAMA, 314(5), 489–500.
Appendix
Evox qEEG scan 1
Baseline Pre Scores
PCL5 Score 1: 74
PHQ9 score 1: 26
GAD7 score 1: 21
Suicidal Ideation: Daily
Global Score: 33
Evox qEEG scan 2
Baseline Post Scores
PCL5 Score 2: 0
PHQ9 score 2: 0
GAD7 score 2: 0
Suicidal Ideation: None
Global Score: 91