
Author: Daniel M. Jarvis
Affiliation: Tactical Resiliency USA / Healing the Hero USA
Abstract
This de-identified case study examines psychological, neurocognitive, and neurophysiological changes in a 68-year-old Hispanic female firefighter-EMT with severe cumulative trauma exposure. Her history included decades of emergency response work and the traumatic loss of her daughter in a motor vehicle crash while simultaneously attempting life-saving measures on her critically injured granddaughter. Baseline psychometric measures reflected severe trauma burden (PCL-5 = 48), severe depressive symptoms (PHQ-9 = 20), and moderate-to-severe anxiety (GAD-7 = 16). Following two sessions of Trauma Resiliency Protocol–Peer Rescue (TRP-PR), post-treatment psychometric scores decreased to zero across all measures.
Objective pre/post assessment using the Evoke Neuroscience platform demonstrated marked gains in global neurocognitive performance (52% to 96%), broad domain normalization, improved processing efficiency, and newly interpretable autonomic data. Persistent areas of recovery need included reduced heart rate variability (HRV) and slowed higher-order ERP processing, suggesting that autonomic recalibration and deeper cognitive integration may continue to improve over time. These findings support meaningful short-term recovery following brief trauma-focused intervention.
Literature Review: Women in the Fire Service and Trauma Exposure
Women in the fire service face repeated exposure to potentially psychologically traumatic events, including fatalities, pediatric trauma, severe injury, moral injury, and chronic sleep disruption. Across first responder populations, clinically significant PTSD, depression, and anxiety are more common than in the general population, with pooled estimates suggesting that 10% to 35% of first responders experience substantial mental health symptoms.
Female firefighters may face compounded risk because occupational trauma often overlaps with organizational stressors such as underrepresentation, discrimination, and role strain in a historically male-dominate (pmc.ncbi.nlm.nih.gov) fighters, approximately 20% screened positive for PTSD symptoms, and nearly 30% reported lifetime suicidal ideation. Women with elevated PTSD symptoms also reported greater depression, anxiety, and functional strain.
Behavioral health reports have also found elevated depressive risk in women firefighters. Prior estimates suggest that 22.2% of female career firefighters and 38.5% of female volunteer firefighters screened at risk for depression. These findings are clinical (pubmed.ncbi.nlm.nih.gov) a burden can impair sleep, reaction time, emotional regulation, and autonomic flexibility.
Recent occupational health research and NIOSH surveillance efforts recognize women firefighters as an underserved population with unique mental and physical health risks. Emerging evidence suggests that anxiety and PTSD may also affect broader physiological recovery, including endocrine and reproductive health markers.
Within (samhsa.gov) occupational critical incidents and traumatic grief may disrupt emotional processing, threat detection, memory retrieval, and autonomic regulation. The present case is clinically significant because it illustrates recovery in a female firefighter-EMT with layered occupational trauma and personal loss following a brief intervention.
1. Background and Trauma Context
Firefighter-EMTs are routinely exposed to repeated high-intensity stressors, including severe injury, pediatric trauma, fatalities, rescue uncertainty, and cumulative grief. Over time, repeated exposure to critical incidents can produce persistent hypervigilance, emotional exhaustion, sleep disruption, autonomic dysregulation, and trauma-linked cognitive inefficiencies.
The participant in this case had a cumulative trauma history that included:
- decades of emergency response exposure,
- repeated exposure to severe injuries and fatalities,
- the traumatic death of her daughter in a motor vehicle crash,
- simultaneous efforts to save her granddaughter at the scene.
This type of layered trauma is consistent with chronic activation of threat detection, emotional memory, and autonomic stress systems.
2. Case Presentation
Participant
- Age: 68 years
- Sex: Female
- Ethnicity: Hispanic
- Occupation: Firefighter-EMT
Presenting Symptoms
Baseline symptoms included:
- intrusive trauma burden,
- depressed mood,
- insomnia,
- headaches,
- emotional overwhelm.
Psychometric Outcomes
| Measure | Pre | Post | Change |
| PCL-5 | 48 | 0 | -48 |
| PHQ-9 | 20 | 0 | -20 |
| GAD-7 | 16 | 0 | -16 |
The participant completed two sessions of TRP-PR between assessments.
3. Method
Measures
- Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5)
- Patient Health Questionnaire-9 (PHQ-9)
- Generalized Anxiety Disorder-7 (GAD-7)
- Evoke Neuroscience neurocognitive screener
- Event-related potentials (ERP)
- Quantitative electroencephalography (qEEG)
- ECG-derived heart rate variability (HRV)
Procedure
The participant completed baseline psychometric and Evoke Neuroscience assessments prior to intervention. She then completed two sessions of Trauma Resiliency Protocol–Peer Rescue (TRP-PR), a structured trauma-processing intervention designed to reduce unresolved emotional intensity without requiring prolonged narrative reliving. Follow-up psychometric and neurophysiological assessments were completed post-intervention.
4. Neurocognitive Recovery
Global Neurocognitive Performance
- Pre-treatment global score: 52%
- Post-treatment global score: 96%
- Net improvement: +44 points
Domain-Level Improvements
| Domain | Pre | Post | Change |
| Memory | 43% | 93% | +50 |
| Executive & Attention | 38% | 96% | +58 |
| Word Fluency | 19% | 100% | +81 |
| Affect | 46% | 100% | +54 |
| Sensory | 79% | 100% | +21 |
| Motor | 96% | 100% | +4 |
Interpretation
The participant demonstrated broad normalization in:
- trauma-related affect regulation,
- executive control,
- language fluency,
- memory retrieval,
- attentional stability.
The most notable gains were in word fluency, executive function, and affect, suggesting significant reduction in trauma-related cognitive interference and emotional burden.
5. Response Metrics and ERP Findings
Response Metrics
| Metric | Pre | Post | Interpretation |
| Reaction Time | 522ms | 495ms | Improved processing speed |
| Response Consistency | 7ms | 8ms | Stable and efficient |
| Omission Errors | 0% | 0% | No lapses |
| Commission Errors | 4.49% | 2.86% | Improved impulse control |
ERP Findings
P300a (Attention / Salience Detection)
- Pre: 508ms, 29.0 microvolts
- Post: 572ms, 55.2 microvolts
Interpretation: The increase in signal power suggests substantially stronger attentional engagement and salience processing. The slower latency may reflect more deliberate and less threat-reactive processing.
P300b (Information Processing / Working Memory Updating)
- Pre: 516ms, 17.8 microvolts
- Post: 628ms, 16.4 microvolts
Interpretation: Working memory updating remained slower than reference range post-treatment. This suggests that while emotional burden improved significantly, higher-order cognitive integration may still be recovering.
N100 (Early Sensory Processing)
- Pre: 244ms, -19.5 microvolts
- Post: 112ms, -4.9 microvolts
Interpretation: Sensory gating speed improved dramatically. However, reduced N100 amplitude post-treatment suggests early sensory response may still be recalibrating. Overall, the pattern is consistent with reduced overload and less hypervigilant scanning.
6. Autonomic Recovery (HRV)
Baseline HRV
The pre-treatment scan did not yield interpretable ECG / HRV data due to artifact, limiting baseline autonomic comparison.
Post-Treatment HRV
| Metric | Post | Reference |
| Heart Rate | 68 bpm | Normal |
| QRS Duration | 0.102 sec | Normal |
| SDNN | 25ms | Low |
| Total Power | 212 ms^2 | Low |
Interpretation
Post-treatment autonomic data were interpretable and showed:
- normal resting heart rate,
- normal cardiac conduction,
- persistent low autonomic flexibility,
- reduced vagal reserve.
Although emotional and cognitive recovery were substantial, HRV findings suggest the participant’s autonomic nervous system remained under chronic physiological stress. This is consistent with long-term cumulative trauma exposure and may improve with time, sleep recovery, and continued regulation work.
7. Quantitative EEG (qEEG) Findings
Pre-Treatment qEEG
Key findings:
- Global score in impaired range (52%)
- theta-to-beta ratio: 1.316 (within range)
- elevated source localization in:
- superior temporal gyrus (+4.8 SD),
- supramarginal gyrus (+4.7 SD),
- middle temporal gyrus (+3.7 SD).
Interpretation
This pattern is consistent with:
- heightened emotional memory activation,
- trauma-linked auditory / sensory processing burden,
- internal replay of distressing experiences,
- affective overload.
Post-Treatment qEEG
Key findings:
- Global score normalized (96%)
- theta-to-beta ratio: 1.459 (within range)
- ongoing frontal / temporal excess activity with EMG artifact noted.
Interpretation
The post-treatment brain maps suggest:
- improved functional organization,
- reduced trauma-linked cognitive inefficiency,
- better overall network performance.
However, persistent frontal / temporal activation indicates:
- ongoing emotional memory processing,
- residual cumulative stress load,
- continued opportunity for deeper integration and autonomic recovery.
This is clinically expected in complex grief and cumulative trauma, particularly after only two sessions.
8. Discussion
This case demonstrated rapid and clinically meaningful improvement following only two TRP-PR sessions.
Key Improvements
- Full remission in self-reported PTSD, depression, and anxiety symptoms
- Global neurocognitive recovery from impaired to optimized range
- Major gains in memory, executive function, and affect regulation
- Faster processing speed and improved response accuracy
- Stronger attentional engagement
- Improved interpretability of autonomic data
Areas Still Needing Work
- low HRV / autonomic reserve,
- slowed higher-order information processing (P300b),
- residual frontal / temporal activation on qEEG.
Clinical Significance
The participant’s trauma history involved layered occupational and personal grief. The magnitude of change after two sessions suggests that TRP-PR may substantially reduce emotional burden and restore cognitive efficiency quickly. At the same time, this case underscores that physiological recovery may lag behind subjective symptom resolution.
9. Conclusion
This de-identified case demonstrates substantial short-term recovery in a female firefighter-EMT following two sessions of TRP-PR.
After treatment, the participant showed:
- complete symptom remission,
- marked cognitive recovery,
- improved attentional stability,
- reduced trauma-linked interference.
Residual autonomic and deeper processing findings suggest continued healing potential. Overall, this case supports TRP-PR as a promising brief intervention for cumulative trauma and traumatic grief in first responders.
Appendix A
Figure A1. Pre-Treatment Evoke Brain Maps
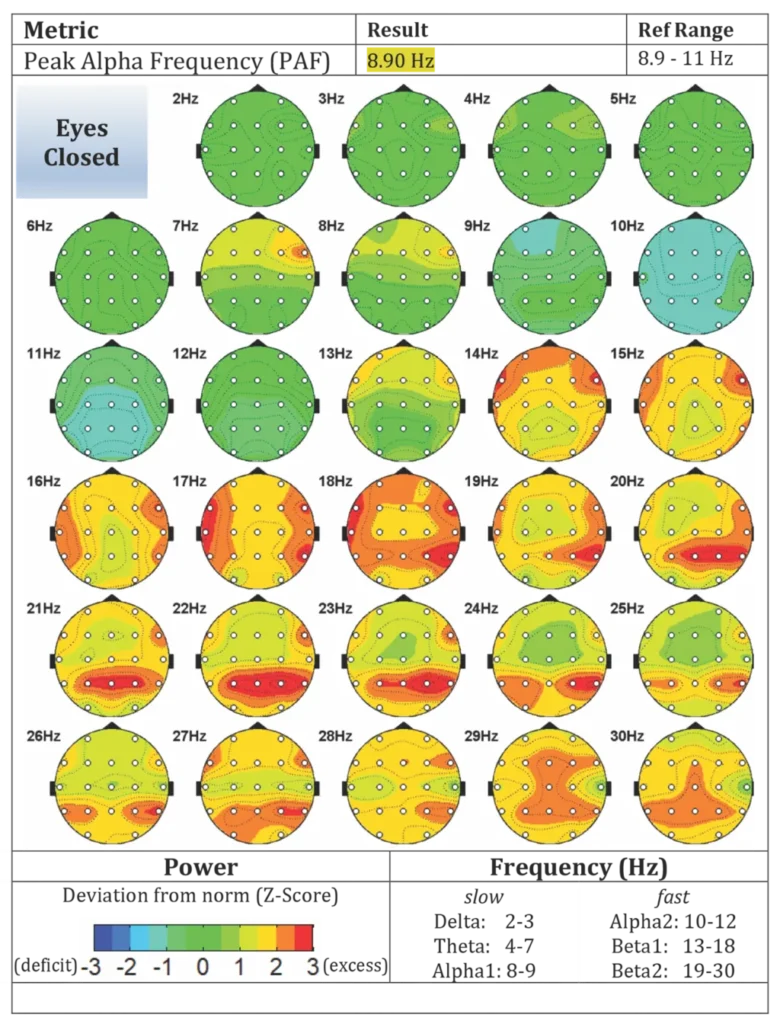
Figure A2. Post-Treatment Evoke Brain Maps
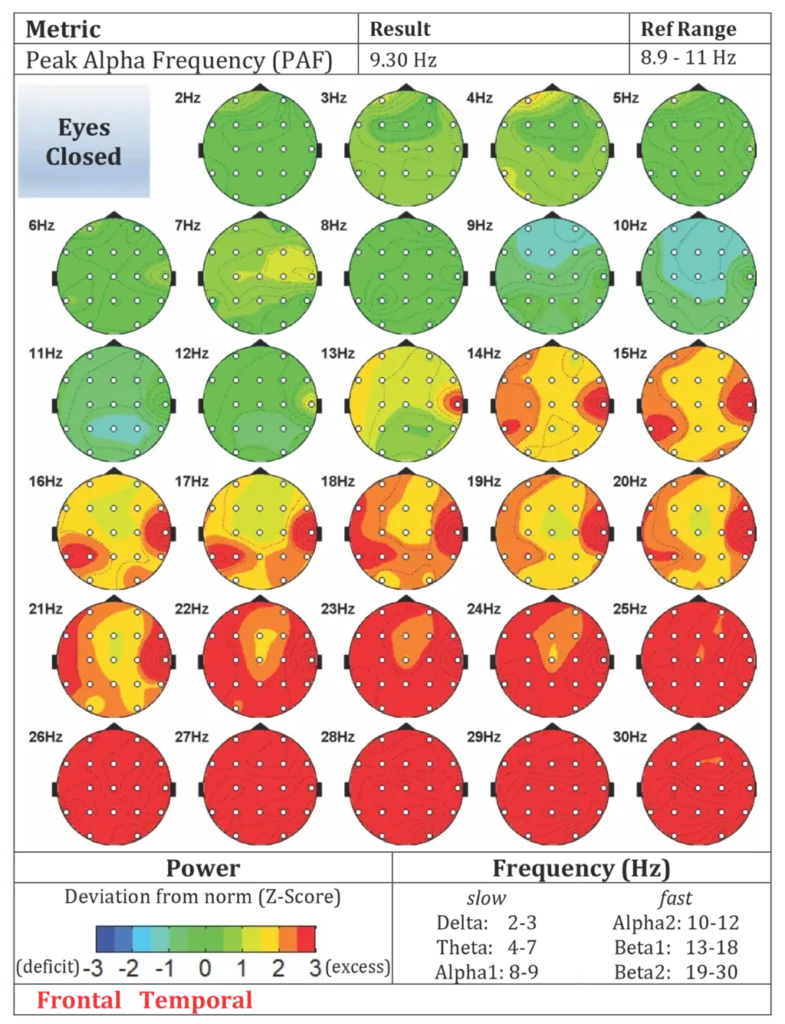
Table A1. Pre- and Post-Treatment Psychometric Outcomes
| Measure | Pre-Treatment | Post-Treatment | Change |
| PCL-5 | 48 | 0 | -48 |
| PHQ-9 | 20 | 0 | -20 |
| GAD-7 | 16 | 0 | -16 |
Table A2. Pre- and Post-Treatment Neurocognitive Outcomes
| Domain | Pre-Treatment | Post-Treatment | Change |
| Global Score | 52% | 96% | +44 |
| Memory | 43% | 93% | +50 |
| Executive and Attention | 38% | 96% | +58 |
| Word Fluency | 19% | 100% | +81 |
| Affect | 46% | 100% | +54 |
| Sensory | 79% | 100% | +21 |
| Motor | 96% | 100% | +4 |
Table A3. Post-Treatment Autonomic Outcomes
| Metric | Post-Treatment | Reference Range | Clinical Interpretation |
| Heart Rate | 68 bpm | 50-80 bpm | Within normal range |
| QRS Duration | 0.102 sec | 0.06-0.12 sec | Normal conduction |
| SDNN | 25 ms | 65-150 ms | Low autonomic flexibility |
| Total Power | 212 ms^2 | >= 800 ms^2 | Reduced vagal reserve |
| VLF:LF:HF | 85:64:63 ms^2 | VLF < LF > HF | Sympathetic predominance |
Appendix Note: The appendix provides visual and quantitative support for the psychometric, neurocognitive, and physiological changes described in the main manuscript.
References
Beaton, R. D., & Corneil, W. (1999). Exposure to traumatic incidents and prevalence of posttraumatic stress symptomatology in urban firefighters in two countries. Prehospital and Disaster Medicine, 14(2), 102–108.
Evoke Neuroscience. (n.d.). Evoke EEG system documentation.
Haddock, C. K., Jahnke, S. A., Poston, W. S. C., Jitnarin, N., Kaipust, C. M., Tuley, B. C., & Hyder, M. L. (2017). Alcohol use among firefighters in the Central United States. Occupational Medicine, 67(5), 366–372.
Jahnke, S. A., Poston, W. S. C., Haddock, C. K., & Murphy, B. (2016). Firefighting and mental health: Experiences of repeated exposure to trauma. Work, 53(4), 737–744.
Jahnke, S. A., Poston, W. S. C., Haddock, C. K., Jitnarin, N., & Day, R. S. (2019). The health of women in the US fire service. BMC Women’s Health, 19, Article 146. https://doi.org/10.1186/s12905-019-0838-4
National Institute for Occupational Safety and Health. (2024). Women firefighters: Occupational health and safety considerations. Centers for Disease Control and Prevention. https://www.cdc.gov/niosh/
Substance Abuse and Mental Health Services Administration. (2018). First responders: Behavioral health concerns, emergency response, and trauma. U.S. Department of Health and Human Services. https://www.samhsa.gov/Stanley, I. H., Hom, M. A., Joiner, T. E., & Spencer-Thomas, S. (2018). Suicidal thoughts and behaviors among women firefighters. Journal of Psychiatric Research, 105, 21–24. https://doi.org/10.1016/j.jpsychires.2018.08.014